 |

Although few teenagers want a pregnancy seven out ten teenaged young men and women become sexually active. Every year about seven out of every hundred young women age 15-19 in the U.S. will become pregnant, (See Timely topics: “Teen Pregnancy”). Compared to most other economically well off countries, teen pregnancy is a major problem for the U.S. Eighty-two percent of the teen pregnancies are unplanned; every year teens account for about one fifth of all unintended pregnancies and 750,000 or 10% of all U.S. births each year are to teenagers [1].
Contraceptive Options: Selecting the Best Ones
Although it might be assumed that unplanned pregnancies are the result of contraceptives not working well, an estimated 52% of unintended pregnancies in the U.S. result from non-use of contraception, 43% from inconsistent or incorrect use, and only 5% because the method itself failed. So finding and using a contraceptive that works and can be used correctly and effectively over time is critical to avoiding unwanted pregnancies [2].
Among teenagers, oral contraceptives, condoms, injectables and withdrawal are the most commonly used methods [3]. While with perfect use these methods are highly effective, because the methods require either remembering to take a daily medication, trips to the pharmacy or clinic for re-supply, or negotiation with partners, 9% of pill users, 18% of condom users, and 6% of injectable (Depo-Provera™) users will become pregnant during the first year of typical use [4].
Contraceptive effectiveness of these methods is also substantially impaired because of high discontinuation rates. About half of condom and injectable contraception users—and almost one-third of pill users—will discontinue use within a year and may become non-users of contraception [4].
Among low-income women in their teens and twenties, contraceptive discontinuation and unintended pregnancy are even more likely. A recent study of a predominantly minority and socioeconomically disadvantaged group of young women found high rates of hormonal contraceptive discontinuation and pregnancy. Less than one-third of initial acceptors of the pill, patch, ring and 3-month injectable were still using the method after a year and between 16% and 30% of the women who had started these contraceptive methods had become pregnant [5].
Risk of unintended pregnancy in the US is therefore closely related to the frequent choice of contraceptive methods that are likely to be used incorrectly or inconsistently. Equally important is the non-use of contraception, either because use was never initiated or because of choosing a method likely to be discontinued shortly after it was adopted.
The figure below groups contraceptives according to effectiveness in preventing pregnancy under typical use conditions. The more effective methods shown in the top row include male and female sterilization, methods that would seldom be appropriate for teens, and IUD’s and implants.
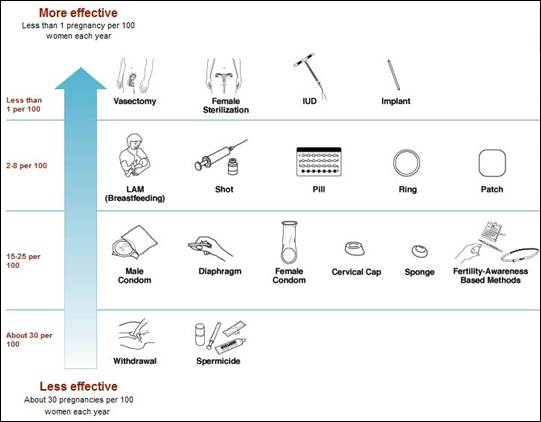
Source: World Health Organization
The Long-Acting Reversible Contraceptive (LARC) Methods
The long-acting reversible contraceptive (LARC) methods are intrauterine contraceptives and implants. Both have a proven record of very high effectiveness, many years of effectiveness, convenience, cost effectiveness, and suitability for a wide variety of women. The LARC methods are an excellent choice for teens. However these methods comprise only 5.5% of contraceptive use in the U.S. [3,4].
The pregnancy rates for the three LARC methods available in the U.S. are very low—they are 99% effective. With typical use, the first year failure rate of the copper T 380A (ParaGard®) is 1%, the LNG-IUS (Mirena®) is 0.1%, and the implant available in the U.S. (Implanon®) is 0.1% [4].
One-year continuation rates for LARC methods are also markedly superior to the short-acting reversible contraceptives at 78% for the copper T 380A, 80% for the LNG-IUS, and 84% for Implanon® [4]. To a large extent, because they do not require continuing motivation and action for use and protection against pregnancy LARC methods have by far the best continuation rates among reversible contraceptives.
The duration of effective action for the copper T 380A (ParaGard®) is 10 years, for the LNG-IUS (Mirena®) 5 years and the implant (Implanon®) 3 years. Although initially expensive, over time IUDs and implants are also the most cost effective among reversible methods [6].
Unfortunately, outdated perceptions about appropriate patient candidates for LARC among health care providers and patients continue to negatively impact their use (7,8,9,10). A substantial body of research has disproved a number of previously presumed contraindications to LARC use. Specifically, women of any age, those who have not had children and those who are seeking contraception immediately after a birth or an abortion are eligible and good candidates for IUDs and implants. Their benefits also outweigh the risks of use in the presence a wide variety of medical conditions such as smoking or high blood pressure that might increase the risk of using the pill or other hormonal contraceptives [10,11,12].
LARC methods therefore are suitable for the vast majority of teenaged women, including those who formerly were thought to be poor candidates for their use and many women using IUDs report satisfaction with the method [11,13,14].
LARC methods also have important health benefits [15,16]. Heavy menstrual bleeding (HMB) is common and extensive evidence indicates that the LNG-IUS is effective in managing HMB due to a wide range of different causes [16]. LNG-IUS use usually improves iron-deficiency anemia [16,17].
Protection against endometrial cancer is a well-documented benefit of copper IUDs. The LNG-IUS is also effective in preventing endometrial changes that precede uterine cancer, preventing its progression, and probably in preventing uterine cancer [16]. The progestin releasing IUD protects against the pelvic inflammatory disease (PID) caused by various infectious agents. The presumed mechanism of action is thickened cervical mucus preventing cervical and vaginal infections from reaching the upper reproductive tract. LNG-IUS users are one-quarter as likely to be diagnosed with PID over 3 years compared to copper IUD users [16].
A reasonable goal is to make high-quality LARC information and services much more available in the U.S. for women of all ages and hope that the proportion of contraceptors choosing those methods will increase to levels seen in France [22%] or Norway [23%], and other European countries with low rates of unintended pregnancy among both adults and teens [3].
References
[1] Finer LB and Zolna MR, Unintended pregnancy in the United States: incidence and disparities, 2006, Contraception, 2011, doi: 10.1016/j.contraception.2011.07.013
[2] Frost JJ, Darroch JE, Remez L. Improving contraceptive use in the United States. In Brief. New York, NY: Guttmacher Institute, 2008, No. 1.
[3] Mosher WD, Jones J. Use of contraception in the United States: 1982–2008. National Center for Health Statistics. Vital Health Stat 23(29). 2010.Table 9 P.26
[4] Trussell J. Contraceptive failure in the United States. Contraception 2011; 83:397-404.
[5] Raine TR, Foster-Rosales A, Upadhyay UD, Boyer CB, Brown BA, Sokoloff A, Harper CC. One-year contraceptive continuation and pregnancy in adolescent girls and women initiating hormonal contraceptives. Obstet Gynecol 2011;117:363-371.
[6] Chiou CF, Trussell J, Reyes R, Knight K, Wallace J, Udani J, Oda K, Borenstein J. Economic analysis of contraceptives for women. Contraception 2003; 68(1): 3-10.
[7] Harper CC, Blum M, de Bocanegra HT, Darney PD, Speidel JJ, Policar M, Drey EA. Challenges in translating evidence to practice: the provision of intrauterine contraception. Obstet Gynecol 2008;111:1359–69.
[8] Fleming K, Sokoloff A, Raine TR. Attitudes and beliefs about the IUD among teenagers and young women. Contraception 2010;82:178-182.
[9] Hladky KJ, Allsworth JE, Madden, Secura GM, Peipert JF. Women's knowledge about intrauterine contraception. Obstet Gynecol. 2011 Jan;117(1):48-54.
[10] Hubacher D. The checkered history and bright future of intrauterine contraception in the United States. Perspect Sex Reprod Health 2002;34:98-103.
[11] Centers for Disease Control. United States medical eligibility criteria for contraceptive use, 2010. MMWR Early Release 2010;59.
[12] Darney PD. Time to pardon the IUD? N Engl J Med 2001;345:608–10.
[13] Peipert, JF, Zhao Q, Allsworth JE, Petrosky E, Madden T, Eisenberg D, Secura G. Continuation and satisfaction of reversible contraception. Obstet Gynecol 2011;117:1105-13.
[14] Forrest JD. US women's perceptions of and attitudes about the IUD. Obstetrical & Gynecological Survey 1996; 51(12): S30-4.
[15] Hubacher D, Grimes DA. Noncontraceptive health benefits of intrauterine devices: a systematic review. Obstet Gynecol Surv 2002;57:120-8.
[16] Fraser IS. Non-contraceptive health benefits of intrauterine hormonal systems. Contraception 2010; 82(5): 396-403.
[17] Suvisaari J, Lahteenmaki P. Detailed analysis of menstrual bleeding patterns after postmenstrual and postabortal insertion of a copper IUD or a levonorgestrel-releasing intrauterine system. Contraception 1996; 54(4): 201-8.
Back to Top
| |

|
|
